
“Mitochondria at 8 a.m. are not the same as at 8 p.m.”: The Chronobiology Secret to Maximizing PBM Effects
Does the therapeutic effect of PBM (Photobiomodulation) depend only on the physical dose (J/cm²), that is, “how much energy you delivered”?
If you’ve applied PBM in clinical practice, you’ve likely seen different results from the same protocol. The key lies in chronobiology.
Modern chronobiology shows that every cell in the body coordinates its metabolism across 24 hours through a network of clock genes. At the moment photons in the 630–850 nm range reach the mitochondria, that cell is already in a specific metabolic state determined by proteins like BMAL1, CLOCK, PER, and CRY.
Here is the critical question:
Will mitochondria at 8 a.m. respond the same way to identical photons as mitochondria at 8 p.m.?
The answer is clearly “No.”
Section 1: Chronobiology Fundamentals — Why Timing Determines PBM Efficacy
1.1 The precise link between clock genes and mitochondria
The master clock gene complex BMAL1/CLOCK drives time-of-day expression of key factors:
- PGC-1α: master regulator of mitochondrial biogenesis
- SIRT1/3: NAD⁺-dependent deacetylases (tune mitochondrial efficiency)
- ROS-detox enzymes: rhythmic expression of SOD2, catalase, and other antioxidants
What does this mean for PBM?
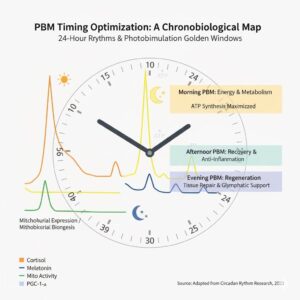
- Morning (6–10 a.m.): Mitochondrial biogenesis pathways (PGC-1α activity) peak. PBM here can maximize ATP amplification.
- Afternoon (2–4 p.m.): A transient metabolic dip occurs. PBM serves as a “bridge” to backfill energy.
- Evening (8–10 p.m.): Recovery and regeneration dominate. PBM can maximize anti-inflammatory and tissue-repair effects.
1.1 The precise link between clock genes and mitochondria
The master clock gene complex BMAL1/CLOCK drives time-of-day expression of key factors:
- PGC-1α: master regulator of mitochondrial biogenesis
- SIRT1/3: NAD⁺-dependent deacetylases (tune mitochondrial efficiency)
- ROS-detox enzymes: rhythmic expression of SOD2, catalase, and other antioxidants
What does this mean for PBM?
- Morning (6–10 a.m.): Mitochondrial biogenesis pathways (PGC-1α activity) peak. PBM here can maximize ATP amplification.
- Afternoon (2–4 p.m.): A transient metabolic dip occurs. PBM serves as a “bridge” to backfill energy.
- Evening (8–10 p.m.): Recovery and regeneration dominate. PBM can maximize anti-inflammatory and tissue-repair effects.
1.2 The background score: cortisol and melatonin rhythms
PBM operates against the backdrop of endocrine rhythms.
- Morning PBM (7–9 a.m.): Morning light entrains the SCN and helps normalize the cortisol awakening response (CAR). Red light at 630–660 nm can engage melanopsin more gently than blue light, making it a good choice to help recalibrate the HPA axis in chronic fatigue.
- Evening PBM (8–10 p.m.): Many worry evening light may impair sleep, but red/NIR PBM, unlike blue light, does not suppress melatonin. It tends to activate the parasympathetic system and improve HRV. One study (J Athl Train, 2012) reported a ~20% increase in circulating melatonin and improved sleep efficiency after 14 days of evening PBM in athletes.
Section 2: Goal-Based Protocol Design — When to Irradiate for What
PBM timing should be decided by why you are applying it.
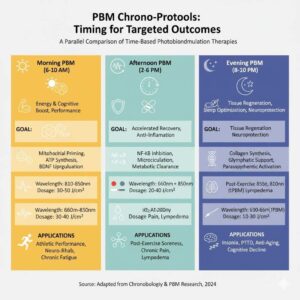
2.1 Morning PBM (6–10 a.m.): Metabolic activation & neuroplasticity (engine warm-up)
Goals: arousal, cognitive performance, peak exercise capacity
Mechanisms:
- Pre-exercise mitochondrial priming: Irradiating at 810–850 nm 20–30 min before exercise increases ATP reserve capacity in muscle and reduces lactate accumulation (Ferraresi et al., 2016). Meta-analyses report ~18.7% average gains in endurance.
- BDNF synergy: Morning baseline BDNF naturally rises; PBM on top of this can enhance synaptic plasticity advantageous for neuro-rehab and cognitive optimization.
2.2 Afternoon PBM (2–6 p.m.): Recovery promotion & inflammation modulation (putting out the fire)
Goals: post-exercise recovery, chronic pain management, DOMS prevention
Mechanisms:
- Anti-inflammatory switch: Post-exercise PBM down-modulates NF-κB, limiting IL-6/TNF-α, while raising IL-10. Reported DOMS reductions of 30–40%.
- Metabolite clearance: NO-mediated microcirculatory improvements accelerate removal of lactate and CK.
2.3 Evening PBM (8–10 p.m.): Tissue regeneration & sleep optimization (system restore)
Goals: maximize nocturnal recovery, support the glymphatic system, improve sleep quality
Mechanisms:
- Tissue remodeling: PBM synchronizes with nocturnal growth hormone (GH) secretion to promote collagen synthesis and remodeling of skin, tendons, and ligaments.
- Glymphatic support: tPBM can increase microvascular pulsatility, facilitating CSF flow and indirectly aiding clearance of waste (e.g., amyloid-β).
Parasympathetic activation: Evening whole-body PBM increases vagal tone and improves HRV in clinical datasets.
Section 3: BAHI Longevity Integration — Time-Synchronized Protocols
The BAHI Longevity philosophy shines in time-synchronized protocols. Body systems do not act in isolation; PBM’s benefits compound when combined with complementary modalities.
3.1 Morning: PBM + EWOT/IHHT (high-octane metabolic activation)
Priming OXPHOS efficiency with PBM, then adding EWOT can amplify oxygen delivery. The aim is synergy well beyond simple addition (e.g., 200–250% vs. 100%).
3.2 Afternoon: PBM + Wave Motion (recovery accelerator)
PBM enhances lymphatic contractility; Wave Motion augments mechanical lymph propulsion. Add hydrogen inhalation (selective antioxidant) to complete the “clear waste + quell inflammation + oxygenate tissues” triad.
3.3 Evening: PBM + hydrogen breathing (neuroprotection & sleep)
While tPBM activates cerebral blood flow and the glymphatic system, molecular H₂ crosses the BBB and selectively scavenges hydroxyl radicals potent for neuroprotection and sleep quality.
| Time Window | BAHI Integration | Target Systems | Clinical Aims |
| Morning (7–9) | PBM + EWOT | Mitochondria + Respiratory | Energy, performance |
| Afternoon (3–5) | PBM + Wave Motion | Lymphatic + Circulatory | Recovery, edema reduction |
| Evening (8–10) | PBM + Hydrogen Breathing | Nervous + Glymphatic | Sleep, neuroprotection |
Section 4: Clinical Practice Guidance
4.1 Chronotypes matter: “Owls” and “larks” need different timing
For early chronotypes, the optimal PBM window may be 30–60 min after wake-up. For late chronotypes, forcing early-morning applications can backfire. Individualize by biological time (e.g., 2–3 h after wake-up), not absolute clock time.
4.2 “More is not better”: the biphasic dose-response
PBM follows the Arndt–Schulz/biphasic curve: low dose = stimulation; optimal dose = peak efficacy; excess = inhibition (for example, cell fatigue, paradoxical tiredness). At signs of over-irradiation (fatigue, headache), reduce dose by 20–30% immediately.
4.3 Consistency beats perfection
A Harvard-linked chronobiology report (Roenneberg et al., 2016) suggests it’s better to apply PBM consistently within a ±2-hour window than to chase the theoretically “perfect” minute sporadically. Predictable light cues are key to clock-gene entrainment.
Section 5: Measurement & Monitoring — How to Confirm Effect
Objective biomarkers
- Acute (immediately post-session): HRV, skin temperature, blood lactate
- Chronic (4–12 weeks): BDNF, VEGF (bloodwork), VO₂max, polysomnography (PSG), cognitive tests (MoCA, Stroop)
Subjective diary
- Energy (VAS 0–10), sleep quality, pain/edema levels, post-exercise recovery speed.
Conclusion: Time is not just a variable—It is a Therapeutic Tool
PBM efficacy is determined by [photon energy] × [the context of biological time].
At 8 a.m. mitochondria are explicitly in ATP-production mode; at 8 p.m. they favor antioxidant and regenerative programs. The same 660 nm photon can trigger distinct biochemical cascades depending on the cell’s schedule.
The BAHI Longevity philosophy integrates this temporal dimension:
- Morning: boot up the energy system (PBM + EWOT)
- Afternoon: support the recovery system (PBM + Wave Motion)
- Evening: optimize regeneration (PBM + hydrogen)
From now on, in PBM protocol design, timing is no longer optional; it is one of the most decisive variables of therapeutic efficacy.











